ATP Production: The Currency of Life and Why Yours Might Be Failing
If you wanted to pick the single most underappreciated molecule in human biology, adenosine triphosphate would be a strong candidate. Your body produces and consumes roughly your own weight in ATP every day. Not metaphorically — literally. Around 60 to 80 kilograms of ATP turn over in the average adult per 24 hours, cycled and recycled through every cell. Everything you experience — thought, motion, immune response, the maintenance of your body temperature, the very fact that you are conscious right now — is paid for in ATP.
And when the supply runs low, the body does not hide it. It simply reduces output.
How ATP Is Actually Made
There are three production pathways, in increasing order of efficiency:
Substrate-level phosphorylation (glycolysis)
Glucose is broken down in the cytoplasm to pyruvate, yielding a small amount of ATP — 2 molecules per glucose. Fast, but inefficient. The pathway works without oxygen.
The citric acid cycle
Pyruvate enters the mitochondrion, gets converted to acetyl-CoA, and feeds the citric acid cycle. This generates a few more ATP molecules but, more importantly, produces high-energy electron carriers (NADH and FADH₂) for the next stage.
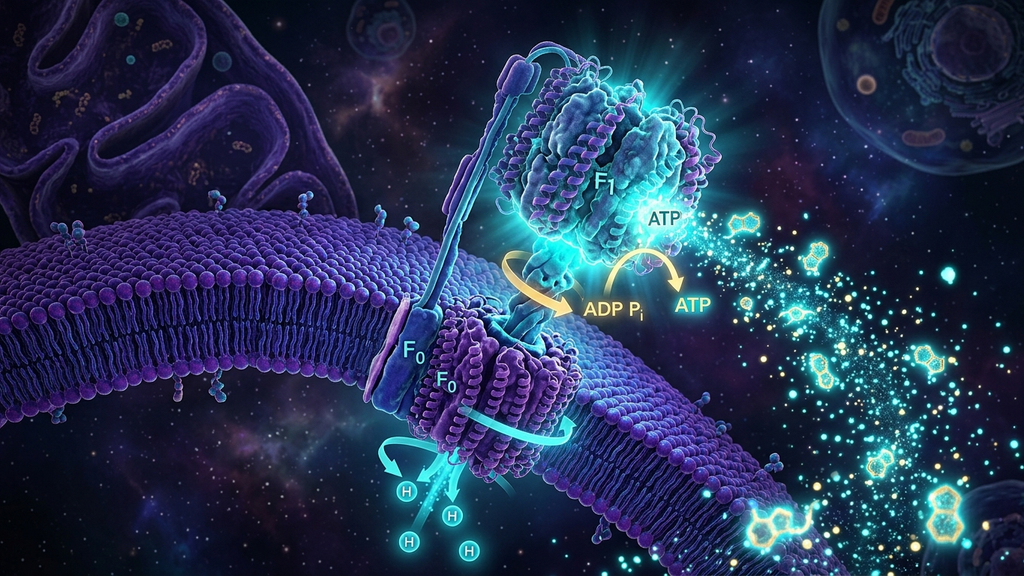
Oxidative phosphorylation
The electron carriers deliver their cargo to the electron transport chain on the inner mitochondrial membrane. The flow of electrons pumps protons across the membrane, creating an electrochemical gradient. ATP synthase — a literal molecular rotary turbine — then uses that gradient to spin and produce ATP. This pathway yields the lion's share: roughly 32 ATP per glucose, and even more from fat oxidation. It is also the most fragile.
What Breaks the System
ATP production fails for surprisingly few reasons. Each, however, can be substantial:
- Substrate shortage. Insufficient glucose, fatty acids, or amino acids — usually a problem only in extreme dietary contexts.
- Oxygen delivery problems. Anemia, hypoxia, severe deconditioning, or microcirculatory dysfunction. Oxygen is the terminal electron acceptor — no oxygen, no oxidative phosphorylation.
- Cofactor depletion. The cycle requires magnesium, B-vitamins (especially B1, B2, B3), CoQ10, iron, and a host of trace minerals. Modern diets and chronic stress combine to deplete these reliably.
- Membrane damage. Oxidative stress, lipid peroxidation, and chronic inflammation degrade the inner mitochondrial membrane. The proton gradient leaks. ATP yield drops.
- Mitochondrial DNA damage. Each mitochondrion has its own small genome. Damage to that genome — from oxidative stress, infections, certain medications — impairs the production of the very proteins the mitochondrion needs to function.
- Reduced mitochondrial density. Sedentary behavior shrinks both the number and size of mitochondria. Disuse atrophy applies to organelles too.
The Clinical Picture of ATP Insufficiency
When the supply chain falters, the body prioritizes. The brain and heart keep getting paid. Everything else suffers visible cuts:
- Fatigue out of proportion to activity
- Exercise intolerance and prolonged post-exertional recovery
- Cold intolerance (thermogenesis is ATP-intensive)
- Cognitive slowing
- Slow wound healing
- Reduced libido and reproductive function (low-priority systems are throttled first)
- Hair thinning and skin changes
- Increased susceptibility to infection
The constellation will look familiar to anyone treating chronic fatigue, long COVID, post-sepsis recovery, or ME/CFS. These are all, in significant part, bioenergetic disorders.
The ATP Recovery Protocol
Step 1 — Audit the Inputs
Iron studies, B12, folate, vitamin D, magnesium RBC, CoQ10 if available. Oxygen saturation. Hemoglobin. Get a full picture of substrate, oxygen, and cofactor availability before reaching for anything fancy.
Step 2 — Stabilize the Autonomic State
Sustained sympathetic dominance increases ATP demand and shunts blood away from peripheral tissues. Slow breathing, cold exposure, vagal stimulation, and adequate sleep are not soft interventions — they reduce ATP demand and improve delivery simultaneously.
Step 3 — Rebuild Mitochondrial Capacity
Zone-2 cardiovascular work, in tolerable doses, is the most reliable driver of mitochondrial biogenesis we know. PEMF and red/near-infrared photobiomodulation appear to support this from a different angle. CoQ10/ubiquinol, magnesium glycinate, B-complex, L-carnitine, and creatine all have a place. In post-viral and ME/CFS patients we layer in NAD+ precursors (NR or NMN), pyrroloquinoline quinone (PQQ), and short fasting windows to stimulate mitophagy where tolerated.
Step 4 — Protect What You Have
Reduce oxidative load (see our companion article on oxidative stress), maintain restorative sleep, and avoid the medications and substances known to inhibit mitochondrial function: chronic high-dose alcohol, statins in some patients, certain antibiotics, and high-dose acetaminophen.
Where Frontier Medicine Is Going
The most exciting work in this space is converging on physical-medicine modalities — ultrasound neuromodulation, PEMF, and photobiomodulation — that appear to stimulate mitochondrial biogenesis without requiring the patient to do strenuous exercise. This matters enormously for severely deconditioned and post-exertional-malaise patients who cannot tolerate the traditional exercise prescription. The mechanisms are still being worked out, but the early clinical signal is consistent: when delivered correctly, these tools can give the system an opening that exercise alone cannot.
Clinical takeaway: Most chronic fatigue is, at root, an ATP supply problem. The interventions that work are unglamorous and slow — substrate, cofactors, autonomic recovery, gentle re-conditioning — but they are also remarkably durable. Treat the energy economy and the symptoms recede.
References
- Wallace DC. "A Mitochondrial Bioenergetic Etiology of Disease." Journal of Clinical Investigation, 2013;123(4):1405-1412.
- Castro-Marrero J et al. "Mitochondrial dysfunction and coenzyme Q10 supplementation in chronic fatigue syndrome." Antioxidants & Redox Signaling, 2015;22(8):679-685.
- Hood DA et al. "Maintenance of skeletal muscle mitochondria in health, exercise, and aging." Annual Review of Physiology, 2019;81:19-41.
- Hamblin MR. "Mechanisms and applications of the anti-inflammatory effects of photobiomodulation." AIMS Biophysics, 2017;4(3):337-361.